Dental cavities frequently target the occlusal surfaces of the molars, which is a significant concern in dental health. The timely detection of these lesions is essential to avoid the need for extensive and complex treatments. Poor identification of cavity lesions can cause unnecessary teeth and a financial burden for the patient (18). Thus, ensuring the precision of the detection of carriers is imperative for general well-being and the satisfaction of patients (19). Consequently, this study was conducted to detect cavities at all steps so that appropriate treatment can be provided.
There are several devices available to detect the first dental cavities, including those based on transillumination, fluorescence and electrical conductance. However, these methods are often sensitive to technique and expensive. In addition, their use of routine in clinical practice requires additional validation and survey. Consequently, the visual examination remains the standard approach to the detection of cavities, in particular for the identification of the cavities of the pit and the crack (18). A literature review has revealed that the visual rating systems currently used, which use DMFT scores, mainly identify cavity lesions. However, studies have shown that ICDAs offer good reproducibility and precision in the detection of occlusal cavities as well as to assess their depth, that the lesions are cavities (20,, 21). However, from a clinical point of view, the inclusion of inactive lesions in the classification of ICDAS is also a question of concern because it can affect treatment decisions (22). Consequently, in this study, we used the ICDAS criteria to detect and assess the progression of cavities.
In this study, to mitigate the biases, two examiners who had undergone training via the ICDAS interactive interactive program before assessing the Caries lesions were recruited. The inter-examination of ICDAS scores, whatever the magnification used, has proven moderate according to the KAPPA test. However, reproducibility has improved considerably when a mild rating criterion has been applied. This confirms that the ICDA online training module effectively educates dental clinicians to understand the rating criteria. This observation aligned with the previous studies carried out by El-Damanhoury et al. (23) and Diniz et al. (24), which has shown that the ICDAS II online learning program improves in particular the diagnostic capacities of caries of dental students as well as graduates. While previous research has indicated the reliability and reproducibility of ICDAs, whatever the previous clinical experience (10,, 23,, 24), our study uniquely incorporated the clinical experience and the knowledge of graduates in the use of a surgical microscope, taking into account the steep learning curve associated with high magnification.
Interestingly, the reliability of the examiners was better when a low threshold for treatment was taken into account for the two magnifications tested. Interestingly, when there was a lower threshold for treatment in different magnifications, there was a better agreement between the examiners concerning reliability. This could imply that a more proactive approach to treatment could lead to clearer consensus among professionals on the actions to be taken, potentially reducing ambiguity or subjective interpretation. This highlights the importance of establishing standardized directives for treatment in diagnostic contexts to improve the coherence and reliability of assessments. In order for enamel cavities to be visible in the form of white spots lesions after drying in the air, the depth of demineralization must exceed 400 μm (25). Consequently, for an ICDAS-II score of 2, where the enamel lesion is clearly visible even when it is humid, the depth of demineralization will be greater than 400 μm. Consequently, non -invasive remineralization therapy can be ineffective, in particular in individuals with a risk of moderate to high cavities (26). Consequently, other studies are necessary to recommend a complete treatment protocol for carious lesions of the non -cavity enamel and to determine the treatment threshold to be applied.
In this study, the histological evaluation suggested by Downer was used as control to assess the extent of dental cavities. Downer's criteria are considered to be the Order to assess the precision of the visual examination in various magnifications because they are easy to understand and easy to use (27,, 28). However, the main concern of histological sections is the inability to visualize cavities in several plans (29). To overcome this, non-destructive methods such as in vitro studies based on micro-CT can better classify cavities in several planes (30). Consequently, additional studies using micro-CT such as the ordered stallion can provide more overview of its diagnostic precision in the detection of cavities.
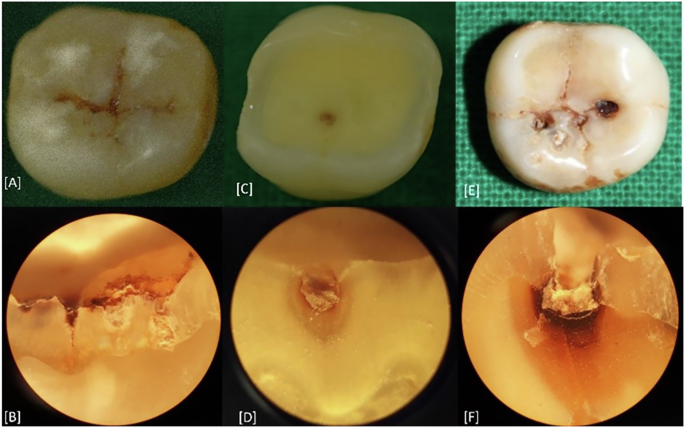
In this study, photographs of the occlusal surfaces of the teeth have been captured and evaluated using the ICDAS system by an expert with more than eight years of experience. These evaluations served as a reference for comparison with direct rating carried out under magnification. Despite vast experience, the diagnostic accuracy of indirect visual methods was not greater than that of the visual examination carried out by novice carried out directly under magnification. This was particularly obvious for codes 0, 1 and 2, because they are recognized as the most difficult to diagnose due to their dependence on the subtle visual changes in intact enamel, which is sensitive to the humidity of teeth (18). Consequently, indirect visual notation can be unreliable even with an experienced examiner, cannot be considered as a viable option. This observation contrasts with the results of the study by Dhanavel et al. (31), which has shown that indirect visual examination had a high sensitivity to detect ICDAS 1 and 2 codes. The difference in results could be attributed to the use of the SOPROCARE intra-oral camera for rating in their study.
A restorative intervention is often necessary when cavities reach dentin. Consequently, in the high threshold intervention group, the operating processing threshold has been set at 3 for histological and ICDAS-II assessments (32). There may be clinical situations where early intervention is necessary, especially for people with a risk of moderate to high cavities. Consequently, in this study, a low threshold group has been introduced, with a 2 -2 intervention cut.
The level of magnification would influence the operator's capacity to detect tiny changes on the surface of the tooth. Consequently, we compared 2 different magnifications, 2.5x (entry -level magnification) and 25x (extreme magnification). Our study revealed that the overall diagnostic precision to higher magnification (25 ×) was lower than that with a lower magnification (2.5 ×), with a greater incidence of false positives. Previous studies have compared the influence of magnification on the operator's capacity (5,, 33,, 34). The influence of different magnification levels, ranging from 2x to 10x, on the diagnostic result when the ICDAS criteria are used have been studied. However, there are no studies on the diagnostic accuracy of extreme enlargement above 25x during the evaluation of occlusal cavities on the basis of the classification of ICDAS.
The binary criterion uses a low threshold for early detection of cavities, while the high threshold is for the early restorative management of cavities. Whatever the threshold of cavities considered, the use of higher magnification has not provided additional advantages in detecting dental cavities in our study. However, sensitivity was slightly better than that at 2.5x. Our present study is in accordance with a previous study by Neuhaus et al. (5), where too high magnification can overestimate the presence of cavities. These results have important implications for clinical decision -making. Excessive dependence on extreme magnification could contribute to unnecessary distribution procedures, increase costs for patients and leading to the premature elimination of the structure of the teeth. Conversely, using an appropriate magnification level, such as 2.5 × magnifiers, can improve diagnostic reliability while minimizing the risk of over-treatment.
A key limitation of this study is that it does not take into account clinical challenges such as saliva, lighting variations and other external factors. Consequently, the results should be validated by additional clinical studies to assess their relevance in practical environments. In addition, future research could focus on assessing the diagnostic accuracy of the ICDAS-II notation system to detect smooth surface cavities in primary and permanent teeth to extend its clinical applicability.